Train with precision and realism using our collection of Surgeon Simulator Models.
Whether for trauma response, surgical skills, or resuscitation practice, each model offers a lifelike learning experience that builds confidence and procedural mastery.
-

SAM 1.4 MK VI
Whole-Body Modular Immersive Simulator Carrier BasProduct Code: SAM 1.4 MK V1The Mk VI male whole-body model includes both upper limbs and non-anatomical “blank inserts” to make the model appear complete. The upper limbs house the left sided SAM 3 Shoulder intra-osseous infusion insert and bilateral SAM 3 Antecubital fossa inserts.
-

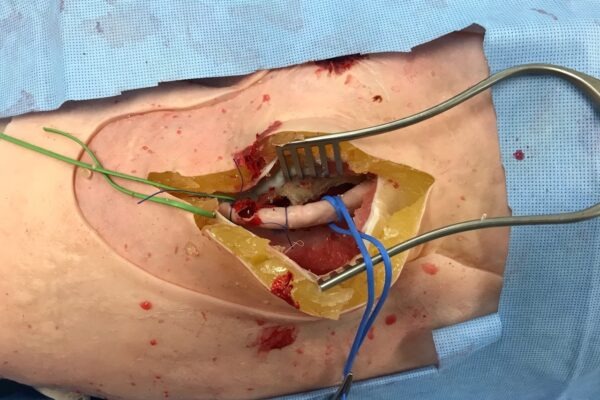
SAM 4P
Pelvic Packing Sub-carrier BaseProduct Code: SAM 4PThis subcarrier base includes representation of the peritoneal sac, bowel, bladder and the aorta, IVC and pelvic vessels. Used together with the replaceable SAM 4.3 Abdo Wall Pelvic packing insert, extra-peritoneal packing can be performed. Further development and inclusion of additional abdominal visceral and structures is underway.
-
SAM 2.1L
Anatomical Left Lower LimbProduct Code: SAM 2.1LThis contains the femur, tibia and skeleton of the foot for fasciotomy and tibial fracture procedures. It can be supplied as a standalone task trainer or along with SAM 1.4 MK VI. Replaceable SAM 2: Lower Left Leg Fasciotomy Inserts are required.
-

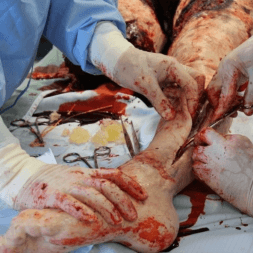
SAM 2.1R
Anatomical Right Lower LimbProduct Code: SAM 2.1RThis contains the femur, tibia and skeleton of the foot for a mid-thigh GSW with arterial injury for control and shunting, an option for femoral fracture and fasciotomies. It can be supplied as a standalone task trainer or along with SAM 1.4 MK VI. Replaceable SAM 2: Lower Right Leg Fasciotomy Inserts and SAM 4.4 Right Thigh Injury inserts are required.
-

SAM 4 MH
Traumatic Amputation And Wound Packing Task TraineProduct Code: SAM 4 MHThis simple to use model allows real-time practice in the control of catastrophic bleeding from lower limb traumatic amputations and cavitated wounds.
-
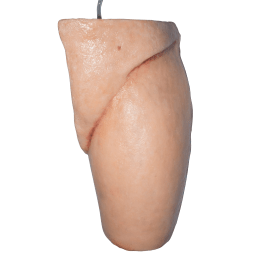
SAM 8
Fascia Iliaca Block (FIB) ModelProduct Code: SAM 8This task training model was originally produced for the RAPID Trial. It allows training in the landmark technique for the insertion of a fascia iliac block. It is not ultrasound compatible, however this is an area of active development.
-

SAM 10 ES
Right Escharotomy ArmProduct Code: SAM 10 ESThe escharotomy arm can be used as a task trainer or attached to the SAM 1.4 MK VI: Whole-Body Modular Immersive Simulator Carrier Base. Developed with support from the Blond McIndoe Foundation, escharotomy of the right upper limb can be performed, with soft tissue swelling into the wound and return of index finger pulp blanching after successful decompression.
-

SAM BS3
Basic Surgical Skills Task Training ModelProduct Code: SAM BS3This simple model allows participants to learn the fundamental skills of skin incision and closure, along with excision of a suspicious naevus and removal of a lipoma.
-
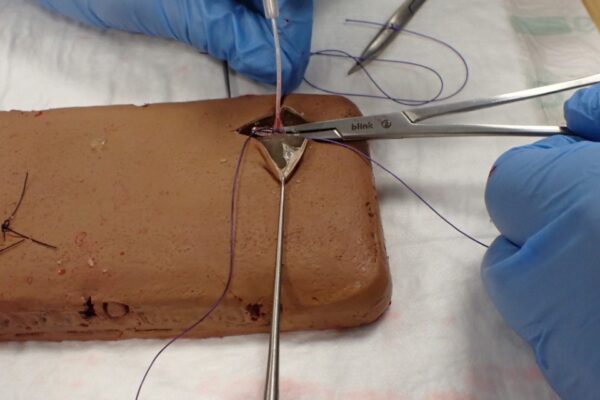
SAM BS-CD
Cut-Down Task Training ModelProduct Code: SAM BS CDAlthough venous cut-down is uncommonly required in current clinical settings, it is a multi-step procedure which provides an excellent vehicle for learning skin incision, soft tissue dissection and ligation of a vein. The model is designed to allow the participant to repeat the steps several times, capitalising on the concept of purposeful properties.
-
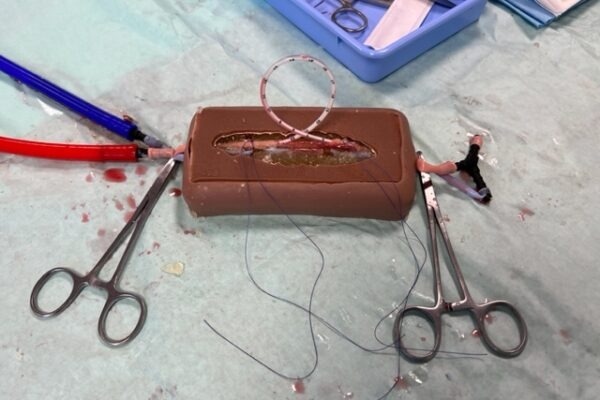
SAM BS-SC
Shunt and Coupler Insertion Task Training ModelProduct Code: SAM BS-SCArterial shunt insertion and use of venous couplers are a standard part in certain vascular and plastic surgical procedures. This model allows both procedures to be practiced, retoring flow through the model.
-
Replaceable Surgical Inserts for SAM 1.4 MK VI
Product Code: SAM 2, SAM 4.1l, SAM 4.2l, SAM 4.4 -

Replaceable Resuscitation Inserts for SAM 1.4 MK V
Product Code: SAM 3, SAM3: AC, SAM 3.1